
The Potential Dietary Intervention to Halt or Prevent Dementia or Reverse the Development of Dementia and Alzheimer's Disease
The comments on the previous web-pages strongly suggest that dietary insufficiency may contribution to the development of the symptomatology associated with Dementia and Alzheimer's disease. To date there have been no definitive trials that have shown that nutrient supplementation can halt or reverse the development of Alzheimer's disease, however, none of the previous trials have addressed the causes as outlined previously. It is hoped that this page can provide a number of potential areas of nutritional supplementation that may be beneficial in the prevention of AD, and possibly halt or reverse early signs of dementia, and prevent dementia.
The current Rate of Dementia at an all-time high: The risk of someone developing dementia in the US is now estimated at one in two. Currently nearly 8 million Americans currently have some form of dementia and there are around 500,000 new cases diagnosed per year. It is postulated that mutations in ApoE are risk factors for dementia, however the rate of the relevant ApoE mutation is only one in 257, so it is highly unlikely that has any major contribution to the 50% of the population destined to get dementia. Hence attention needs to concentrate on modifiable factors. Identified risk factors include less education, hearing impairment, smoking, depression, physical inactivity, traumatic brain injury, high blood pressure, social isolation, air pollution, diabetes, obesity, high cholesterol and excessive alcohol consumption. Lack of or poor sleep is also a risk factor. Of these high blood pressure, diabetes, and obesity can be due to functional B2 deficiency, whilst high cholesterol and poor sleep are due to functional B12 deficiency. Functional B2 deficiency (due to Iodine, Selenium and/or Molybdenum deficiency) causes functional B12 deficiency, leading to elevated homocysteine, nerve demyelination, reduced production of creatine, lower production of CoQ10, lower production of acetylcholine, elevated cholesterol, lower activity of aconitase, and succinic anhydride, all typical of AD.
Lowering Homocysteine: Clearly lowering homocysteine is desirable. This can be achieved through dietary intake of sufficient folate, vitamin B6, iron, vitamin B2 (plus Iodine, Selenium and Molybdenum) and vitamin B12. In individuals with suspected hypothyroidism this should be treated/corrected and dietary iodine, selenium and molybdenum included or supplemented. Treatment of vitamin B12 this is a little bit more difficult as once a person becomes deficient, it is very hard to achieve sufficiency through diet. Further, many people do not gain benefit even from injection of the provitamins cyanocobalamin or hydroxocobalamin and so mixed adenosyl/methyl cobalamin supplementation would be desirable. There have been many oral supplementation trials examining the effect of high dose cyanocobalamin and folate +/- other B group vitamins on lowering homocysteine and attempting to increase the Mini-Mental State Examination (MMSE) scores (reviewed in (1)). Whilst some of the trials were successful in lowering homocysteine no trial using oral supplementation achieved an increase in MMSE. Despite this the trials have been repeated over and over again, and in an almost "Ground hog" like fashion have repeatedly administered oral high dose cyanocobalamin and folate +/- other B groups, and expected or hoped for a different result. Further the importance of functional vitamin B2 in the cycling of both folate and vitamin B12 has been almost completely over-looked in all reviews. Thus, the lack of success following orally administered mixtures of folate, vitamin B12 (the inactive cyanocobalimin analogue), plus vitamin B6, is totally expected, firstly because the delivery of vitamin B12 to the brain is exceedingly difficult and secondly the amount of vitamin B12 taken up from the gut is very low, and third, functional vitamin B2 sufficiency is essential for maintenance of vitamin B12 activity. In line with what is known about the blood-brain barrier, even the smallest of water soluble molecules is actively excluded from entering the brain. Further, even with the injection of radiolabeled vitamin B12 derivatives less than 0.01% of the dose reaches the brain. Little wonder then that the very limited uptake that is achievable from oral delivery of vitamin B12 has been found to be totally ineffectual in "loading" up the brain.
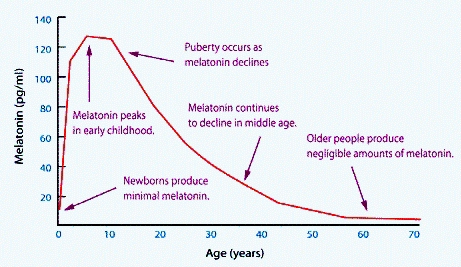
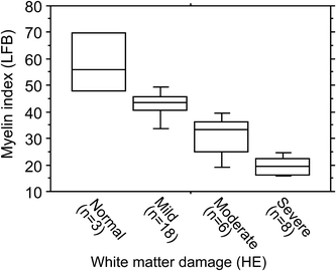
Vitamin B12: Vitamin B12 plays a critical role in myelination, both in the provision of the methyl group for methylation of myelin basic protein and also in the correct processing of methyl malonic acid. Vitamin B12 lack has been associated with incorporation of faulty lipids into the myelin sheath and in the production of faulty myelin basic protein, and destruction of the myelin sheath is a feature of vitamin B12 deficiency. Formation of melatonin requires methylation, and maintenance of the myelin sheath requires melatonin and vitamin D. Levels of Melatonin decrease with age. Demyelination is a feature of Alzheimer's disease, and loss of myelinated axons has been found in AD(2).
Overt vitamin B12 deficiency is correlated negatively with cognitive functioning, and is associated with memory impairment, slowness of thought, attention deficits and dementia (3,4,5). It is also associated with decreased nerve conduction velocity (6).Whilst overt B12 deficiency is easily defined levels of B12 even as high as 350 pmol/L have been associated with brain shrinkage, which has also been shown to be associated with cognitive decline (7,8). It would therefore appear logical to maintain vitamin B12 levels that are considerably higher than this. The close relationship between folate and vitamin B2 with maintaining methyl B12 levels, would intimate that it is also essential to maintain adequate levels of these two vitamins as well. In this regard, it has been shown that supplementation with folic acid, vitamin B6 and vitamin B12 was able to slow brain shrinkage in elderly subjects with increased dementia risk (8,9,10,11,12). Unfortunately they did not go further and also supplement with vitamin B2. This is despite the fact that functional vitamin B2 has been known to be essential for maintenance of functional vitamin B12, particularly methyl B12, for over 50 years yet review after review and study after study fails to acknowledge or account for possible lack of functional B2 activity. Despite this study after study, funded by grant after grant has been performed and has not included any of B2/I/Se/Mo in the protocol. To date we could find only one supplementation study has been performed with B2/B12/folate, in combination with Iodine, Selenium and Molybdenum, all three of which are required for formation of the two active forms of vitamin B2, viz FMN and FAD (13). There was however, no change in cognitive functions found following supplementation, possibly due to the use of selenomethionine as the source of selenium. Selenomethionine has repeatedly failed to change markers of vitamin B2 activation in our hands. Vitamin B12 supplementation is also warranted due to the role of Methyl B12 in the formation of choline and the findings of greatly reduced levels of B12 in the brains of elderly persons (14). Vitamin B12 intake should equal or exceed 6 ug/day in persons who do not have other underlying complications, such as sub-optimally treated hypothyroidism, use of PPIs, GORD medication, pernicious anaemia, use of MetforminTM medication, the presence of atrophic gastritis, or other B12 modifying conditions. It should also be noted that it is highly unlikely that orally administered vitamin B12 would ever deliver sufficient B12 to overcome deficiency in the brain. First, the amount of B12 taken up from the gut is maximally 6-10 ug, and of this less than 0.1% ever reaches the brain. In these cases higher supplementation should be attempted either by injection or by other high supplementation methods, such as transdermal application.
It should be noted, that successful cycling of vitamin B12, particularly methyl B12 requires functional vitamin B2, which in turn requires adequate intake of Iodine (150-300 ug/day), selenium (55-200 ug/day) and molybdenum (100-200 ug/day). I/Se/Mo are not normally incorporated in most multi-vitamin formulations, although this is changing. In this regard, the two main enzymes that support vitamin B12 cycling are both B2 dependent, viz: MTHFR and MTRR. The activity of both enzymes has been shown to be critically dependent upon riboflavin status, and a dramatic drop in activity is seen in the two common variants of MTHFR (677C>T) and MTRR (66A>G) in suboptimal riboflavin concentrations (15). It is surprising, then, that supplementation studies have not addressed these probable deficiencies, particularly since the frequency of these mutations is very high.
More recently, the incidence of Paradoxical B12 deficiency has risen dramatically. In this condition levels of serum vitamin B12 may be normal or elevated, however, markers of functional vitamin B12 deficiency are also elevated - a situation of Paradoxical B12 deficiency.
Rate of brain atrophy has been slowed by ultra-high dose administration of a mixture of L-methylfolate, methylcoblamin, and N-acetyl cysteine (16) administered by injection.
Successful reversal of fronto-temporal dementia has been reported in an elderly gentleman who was given repeated injections of high dose vitamin B12 (17). Whilst broad neurological disorders, including poor Hasegawa dementia scale ratings were greatly improved by supplementation with high dose injected methylcobalamin (18). Similarly improvement in cognitive function was also achieved by intravenous methylcobalamin (19).
MethylB12 due to its role in recycling homocysteine, methionine and eventually S-Adenosylmethionine, also has a critical role in the production of creatine, and creatine-phosphate, and also in the production of ubiquinone. Lack of production of creatine, and/or ubiquinone have both been correlated with lower cognitive function and intellectual disability. Serum coenzyme Q10 have been found to be inversely associated with the risk of disabling dementia. For some reason, methyl-B12's critical role in the production of these very important energy related molecules has been missed by all but a few who work in the field.
Melatonin levels are also dependent upon methyl B12, due to the role of methylation in the conversion of serotonin to melatonin. Melatonin has been shown to have a very important role in maturation of myelin producing oligodendrocytes (20), and in promoting myelination during development and after neuronal damage (21,22,23,24,25). This activity would be compromised in vitamin B12 deficiency and would contribute to the observed reduced myelin sheath thickness characteristic of the aged brain. (see above).
Maintenance of functional vitamin B12 requires not only daily ingestion of vitamin B12, but also vitamin B2, Iodide (150 ug/day), Selenium (as Selenite, 55 ug/day), and Molybdenum (100 ug/day).
Selenium: Recently, a very encouraging study was carried out using sodium selenate at a quite high concentration (0.32 mg and 3.0 mg qdx3) (26). In the 24 weeks study, brain selenium concentration was raised and MMSE did not fall when compared to controls. Other biochemical markers were not reported. Sodium selenate supplementation of mice reversed hippocampal-dependent learning and memory impairments (45) It must be noted that studies with selenomethionine have not been shown to affect MMSE.
Iron: Supplementation with heme iron or addition of iron containing foods may be of benefit. Measurement of iron deficiency as per levels of serum ferritin is highly controversial, but it is generally agreed that iron deficiency anaemia occurs at around 20 ug/L ferritin, mild iron deficiency initiating symptoms such as restless leg syndrome occurring at round 50 ug/L with some evidence of iron deficiency occurring between 50-100 ug/L. Evidence of reduced mitochondrial energy output is definitely apparent at levels below 70 ug/L ferritin. Data looking at ferritin levels, in individuals where one would assume maximum benefit from iron would be desirable, have shown that the highest performing athletes had levels of between 80-185 ug/L (mean 134 ug/L)(2). Iron intake should equal or exceed 9 mg/day for men and post-menopausal women. Studies looking at chronic heart failure suggest that levels below 100 ug/L ferritin are of potential risk. It is apparent that as iron levels decrease, iron is lost from muscles, brain and heart, and lack of iron in muscles can account for the frailty, which is characteristic of dementia. The enzyme, aconitase starts to uncouple when ferritin levels are lower than 50 ug/L, and the activity of the Electron Transport Chain decreases as levels of iron decrease. Vitamin B12, through its action on the sulphation pathway is essential for the formation of iron-sulphur (Fe-S) clusters, and these are essential elements of aconitase (in Krebs cycle), and there are multiple Fe-S clusters in Complex I, II and Complex III of the Electron Transport Chain. Fe-S clusters are also essential for processing Molybdenum, and the formation of the Molybdenum cofactors in enzymes such as sulfite oxidase, xanthine dehydrogenase, aldehyde oxidase, and miochodrial amidoxime reductase. Intracellular processing of iron requires FAD (from B2), and GSH.Without these the soluble Fe2+ form of iron is readily oxidized to Fe3+, which is insoluble and can precipitate within the cell, adn cause ferroptosis. Ferroptosis is a feature of diseases such as AD, PD
Aconitase: Aconitase is arguably one of the most important enzymes in the citric acid cycle, and reduced activity of the enzyme, due to lack of formation of iron-sulphur complexes will lead to a greatly decreased energy output by the mitochondria. Enzymatic activity has been shown to be reduced in conditions of sub-optimal iron concentrations and sub-optimal sulphur concentrations. Increasing levels of iron/ferritin and conditions that increase the processing of sulphur from dietary methionine, should favour increased aconitase activity. The inflection point for loss of aconitase activity is around 70 ug/L ferritin, which is considerably higher than many pathology laboratories would "flag" as deficiency. Thus, potentially many individuals with sub-optimal iron levels are not being treated for non-anaemic iron deficiency. Thus, maintenance of sufficient iron in the diet, plus intake of sulphur in the form of methionine, and ensuring sufficient vitamin B2 and vitamin B6 would all help to provide sufficient iron and sulphur to maintain the activity of aconitase. In addition it has been shown that elevated production of S-Adenosylmethionine (SAM) is required in order to move sulphur from the methylation cycle to the sulphation cycle for incorporation into Fe-S proteins. This further predicates the maintenance of high levels of active vitamin B12, sufficient folate and active vitamin B2.
Hydrogen sulfide: Given that generation of H2S occurs as a result of processing of homocysteine by the enzyme cystathionine beta synthase, conditions that increase the processing of homocysteine by CBS will also increase the production of CBS, viz: increased iron, B6 and B2, and increased dietary methionine, elevated vitamin B12, and sufficient folate.
Acetylcholine: Studies examining plasma phosphatidylcholine docosahexaenic acid (DHA) showed that those who had a higher mean intake of DHA had a significant (47%) reduction in the risk of developing all-cause dementia (20). This is in contrast to studies in which lecithin supplementation did not affect the risk of development of dementia (21). Dietary supplementation with egg yolk phosphatidylcholine has shown memory improvement in models of AD (22). Once again supplementing with methyl B12, folate and vitamin B2 should increase methylation and formation of choline and acetylcholine, which should help to reduce the rate of degeneration of cholinergic neurons, which is a feature of AD (27,28,29).
Increased blood supply to the brain: The mantra for preventing AD has for a long time been "diet and exercise", however, the benefits of this are generally not explained. Evidence suggests that there is restricted blood supply to the brains in AD, and the thought is that increasing the exercise regime will increase the blood supply to the brain. There is potentially a nutritional way to increase blood supply to the brain and that is by providing iron, FMN/FAD and BH4 for increasing the activity of the enzyme, NOS. Increased generation of the vasodilator nitric oxide by eNOS, has been shown to increase cognitive function (30). Aberrant NOS activity is a feature of AD (31). Reduced NOS activity has also been shown to increase the formation of amyloid precursor protein (32). Boyle and co-workers (33) found a correlation between lack of physical activity, increased weight and brain atrophy in AD. Somewhat at odds with this finding was the lack of correlation between elevated systolic blood pressure and dementia in those above 80 (34).
Vitamin D: As discussed previously Hypovitaminosis D, is associated with brain changes and an increased risk of dementia, further it has even been found that vitamin D supplementation can slow, prevent or improve neurocognitive decline (42). It would therefore appear obvious that persons should make sure that they obtain plenty of vitamin D, either through sun-exposure or through diet, and that they should maintain sufficient iron/vitamin B2/vitamin B12 in order to activate vitamin D to its active form 1,25-diOHD (Calcitriol). Avoid using extremely high SPF cosmetics, which have now become the "norm". Suggested levels of calcidiol are above 75 ng/ml. In addition, due to potential vitamin D lowering effects of statins, it would be prudent to avoid their use.
Lack of vitamin D has also been associated with a loss in hippocampal volume (an area of the brain that regulates motivation, emotion, learning and memory), and hence low vitamin D would be associated with difficulty learning. Low vitamin D has been associated with cognitive decline in adults (Wentz etal, 2014). Low vitamin D in utero has been associated with autism spectrum disorder and schizophrenia (Eyles etal, 2013; Ali etal, 2020, 2018), whilst in adults it has been associated with depression and Alzheimer's disease Littlejohns etal, 2014; 2016; Dickens etal, 2011).
The importance of sun-exposure for the production of vitamin D has been known 1822 (nearly 200 years), and particularly exposure to UVB radiation (290-315 nm) (Holick 2006). However with the advent of sun-protection factors in the early 1870s, and the addition of high SPF value cosmetics and the increase in hours worked indoors, plus various sun-avoidance practices has seen a rise in the incidence of vitamin D deficiency, and an increase in the incidence of rickets with the result that vitamin D deficiency in children has once again reached epidemic proportions (Holick 2006). One of the potential sources of vitamin D is dairy, and so, the reduction in the consumption of dairy products, particularly those from free range cows and the switch to alternative products such as soy, and almond drinks, and adoption of a vegan diet can further reduce vitamin D levels.. Vitamin D deficiency is very common in some countries, and over 42% of Singapore residents (92), 45.5% of Saudi residents, and in 2018 over 82.5% of females in South Korea (an increase from 76% in 2008)(93) were found to be vitamin D deficient. Patients with vitamin D serum levels of <25 mg/ml had an increased risk of developing Alzheimer's Disease in comparison with those >25 mg/ml. Severe deficiency had the strongest association. Vitamin D has been shown to prevent cognitive dysfunction via neuroprotection, neurotrophy, neurotransmission, and neuroplasty. Rates of vitamin D sufficiency have fallen by 40% over the past 10 years, which is inversely proportional to the doubling of the incidence of Alzheim's disease from 60/100,000 to 120/100,000 in the UK (
Mode of activation of Vitamin D in the brain, following stimulation of the eye by 482 nm light.
"Nexus Theory™" and Dementia: Recently, it has become apparent that activation of vitamin D to form the active form, calcitriol, is not quite as simple as one would imagine. Thus, whilst most enzymatic reactions only involve the activity of one enzyme, the conversion of 25-hydroxy-vitamin D to the active form 1,25-dihydroxyvitamin D (calcitriol) involves a multi-enzyme complex, which consists of CYP27B1 (25-hydroxyvitamin D3 1-alpha-hydroxylase), Adrenodoxin (an Iron-sulphur protein) and Adrenodoxin reductase (an NADPH/.FAD enzyme). Generally this activity is performed in the kidney, but it has been found that a similar assembly system exists in the brain. Thus, there is a joining or Nexus of enzymes requiring vitamin D, Iron, vitamin B2 (as FAD), and an iron-sulphur complex, wherein the sulphur for such complex is critically dependent upon the activity of the methylation cycle as ipso facto, methyl vitamin B12. A corollary to the "Nexus Theory™ is that any attempt to reverse the damage that has occurred in the early stages of the development of dementia, must address all of the above deficiencies, because if it does not such attempts will not succeed. Further, when one considers the multi-component nature of the "Nexus Theory™", one can see how so many known deficiencies contribute to the condition. Thus, Vitamin D (as 1,25 dihydroxyvitamin D - the active form) has a critical role in remyelination in damaged nerves and in the initial myelination of nerves, and in the processes involved in "neuronal plasticity". Oligodendrocytes (the cells that make the myelin sheath) are stimulated to produce myelin by binding active vitamin D. This then works in concert with melatonin (a methylation dependent hormone) to stimulate mitochondrial energy production in neurones, and to activate the oligodendrocytes. The "Nexus Theory™ of Dementia thus encompasses the known deficiencies associated with dementia, including lower folate, lower vitamin B12, elevated homocysteine, lower iron(42, 43), lower selenium (43, 44), lower Molybdenum (42), and lower vitamin D.
Summary: Looking at the above solutions it is apparent that if there single nutrient deficiency, specifically active vitamin B2, the activity of the other nutrients, vitamin B12, iron, folate and vitamin B6 will be compromised. This is very similar to the nutrient suggestions suggested by the works of Douaud (9) and de Jager (10), who have demonstrated the effectiveness of folate, vitamin B12 and vitamin B6, with the addition of heme iron and vitamin B2. Curiously, lack of the single nutrients selenium (55 ug/day) or molybdenum (100 ug/day) or iodine (150 ug/day), could have similar effects due to their importance in the generation of active B2 (FAD). Similarly, lack of vitamin B12 (6 ug/day), due to it's role in folate processing, reducing homocysteine, stimulation of SAM, with resultant movement of sulphur from methionine into the synthesis of iron-sulphur porteins, and the resultant increase in energy production by the citric acid cycle through aconitase activity. Apart from the nutrient suggestions, it is generally accepted that obesity and lack of exercise both are associated with a higher incidence of AD. Hence it would appear that a diet that is nutrient rich and calorie sufficient, when combined with moderate amounts of cardiovascular exercise, may be of considerable benefit to those wanting to prevent, halt or even reverse the "dementia" process.
Early Detection of Dementia and Alzheimer's Disease
The probability that one can reverse the symptoms of dementia and thereby prevent the onset of Alzheimer's Disease would depend upon finding a way to detect early symptoms of the disease. Given that Alzheimer's Disease is regarded as a classical mitochondrial disease, then assays that can determine the functional activity of the mitochondria should be beneficial.
Potential assays include
(i) direct measurement of aconitase function
(ii) measurement of organic acids in urine, or metabolic analysis.
Currently Great Plains laboratory performs an Organic Acids Test (http://www.greatplainslaboratory.com/organic-acids-test/ ), whilst a similar metabolic test is also carried out by Genova (https://www.gdx.net/product/metabolic-analysis-test-organic-acids-urine ). Both of these tests are capable of identifying metabolic deficiencies that could ultimately lead to dementia/AD.
(iii) measurement of iron status. Steady decline in serum ferritin levels would be indicative of potential problems and could be addressed relatively easily. Experience has show that once serum ferritin levels drop below 70 ug/L, energy production from aconitase starts to drop. This level of ferritin will not however be "flagged" by pathology laboratories whose sole measurement relates to iron deficiency anaemia, rather than to impending energy loss and functional loss of actonitase and succinate dehydrogenase activity.
(iv) falling serum vitamin B12. Falling functional vitamin B12 can be monitored by measuring an increase in the metabolic products MMA and homocysteine. The so-called "active B12 assay" is a complete misnomer, however falls in serum B12 and/or active B12 are representative of loss of total vitamin B12 in serum. Loss of functional vitamin B12 in the brain precedes loss in serum.
(v) reduced production of Ubiquinone. Falling functional vitamin B12 can be monitored by measuring reduced production of Ubiquinone and hence reduced energy output in the electron transport chain. Synthesis of Ubiquinone (CoQ10) requires 3 methylation steps during synthesis, hence lack of methylation due to low methyl B12 levels reduces energy output due to lack of production of CoQ10. A corresponding increase in the levels of 3-hydroxymethylglutarate is seen in the urine. Use of statins also reduces the levels of CoQ10 is detrimental to energy production.
Lifestyle and Dementia and Alzheimer's Disease
It is known that there are at least seven modifiable facts that increase the risk of dementia.
These include, smoking, obesity, high blood pressure (hypertension), inactivity, diabetes, depression and poor education. Of these, obesity, high blood pressure (hypertension) and diabetes have all been shown to potentially be caused by low vitamin B2 in the diet. Further, the level of obesity has been shown to be inversely related to functional vitamin B12 levels and lower activity of aconitase, resulting in lower energy output (34).
Regular exercise that raises the heart rate can increase the flow of blood to the brain, and so reduce the risk of dementia. The exercise has to be intense and increase cardiovascular fitness, as well as increasing the both the muscle mass and muscle strength (35). Additional benefit has been achieved with resistance training (36). Furthermore, regular exercise can also help to reduce the risk of developing dementia as it can help to reduce weight, decrease blood pressure and decrease the risk of diabetes.
Being socially engaged, and participating in activities that stimulate the brain, such as mental challenges and learning new skills, languages, or advanced learning are all associated with a lowered incidence of dementia.
Protect your brain from damage. There are many instances where AD has arisen soon after a mild or severe injury to the brain.
Avoid medications that can affect the uptake and processing of nutrients, including antacids (Prilosec, Nexium, Zantac, Prevacid, Ranitidine, Famotidine, Nazitidine, Cimetidine, etc), and MetforminTM. Avoid bariatric surgery, including bowel resection or gastric by-pass surgery, as well as gastrectromy, particularly of the cardiac or fundus.
Avoid the use of statins. Statins block the enzyme HMG-CoA-reductase, and in so doing reduce the production of precursors involved in the production of ubiquinone, and increase the potential energy output in the electron transport chain and also increase the risk of cardiovascular disorder, depression and heart failure (37)
Further information on preventing and early detection of diabetes can be found on many sites, of which the following is but one (PreventingType2diabetes).
Brain Training and Alzheimer's Disease Prevention
There are several indications that exercising the brain can delay the onset of AD, and George Mears from the Brain Wellness Institute (see info@brainwellness.info) has kindly submitted a summary of the latest suggestions for preventing dementia. These suggestions can be found in the attached document. The mechanism whereby the "Brain Training" may have some effect may be as a result of the dopamine reward from successful training experiences. It is known that there is an age related loss of dopaminergic cell bodies in the brain (39), and at least one study has shown that brain training is associated with changes in the density of cortical dopamine D1 receptors (40).
Diet and Alzheimer's Disease Prevention
It is often said that a diet that is good for the heart is good for the brain, and that the best example of such a diet is the Mediterranean diet. More careful analysis reveals that the diet is one of high nutrient density.
Whole grains, brown rice and whole wheat pasta - providing vitamin B1, molybdenum and iodine
Nuts, seeds and beans - providing selenium, molybdenum, manganese and folate
Fresh fruit and vegetables - providing folate and magnesium
Fish, poultry, eggs, some red meat, clams, oysters, and mussels - providing zinc, iodine, selenium, biotin, iron and vitamin B12
Milk, cheese, and yoghurt - providing calcium, vitamin B2 and vitamin D.
Diets containing sufficient amounts of vitamin B1 and vitamin B2 can also reduce the risk of diabetes (a preventable risk factor for dementia), due to better blood glucose control.
Diets high in Iodine, Selenium and Molybdenum provide support for activation of vitamin B2 - and essential co-factor for the activation of vitamin B12, vitamin D, iron and metabolism of glucose and fats.
Studies on diets and healthy aging
Further data on diets and healthy aging can be found by looking at the following studies on aging
The Seven Countries Study http://www.sevencountriesstudy.com
Lyon Diet Heart Study http://circ.ahajournals.org/content/circulationaha/99/6/779.full.pdf
PREDIMED Study http://www.nejm.org/doi/full/10.1056/NEJMoa1200303
DASH Diet http://dashdiet.org/
MIND Diet https://www.ncbi.nlm.nih.gov/pubmed/16086182 https://www.ncbi.nlm.nih.gov/pubmed/25681666
References
-
Fang, M., Hu, J., Weiss, J. et al. Lifetime risk and projected burden of dementia. Nat Med (2025). https://doi.org/10.1038/s41591-024-03340-9
-
Clarke etal, 2014 Effects of homocysteine lowering with B vitamins on cognitive ageing: meta-analysis of 11 trials with cognitive data on 22,000 individuals. PMID: 24965307
-
Habte etal, 2015 Iron, folate and vitamin B12 status of Ethiopian professional runners. PMID: 26719754
-
Scheltens etal, 1995 Histopathologic correlates of white matter changes on MRI in Alzheimer's disease and normal aging. PMID 7746401.
-
Wynn and Wynn, 1998 The danger of B12 deficiency in the elderly. PMID 9836201
-
Bottiglieri 1996 Folate, vitamin B12, and neuropsychiatric disorders.PMID 9155210
-
Briani etal, 2013 Cobalamin deficiency: clinical picture and radiological findings.PDF
-
Misra etal, 2003 Vitamin B12 deficiency neurological syndromes: a clinical, MRI and electrodiagnostic study. PMID 12613142
-
De Jager, 2014 Critical levels of brain atrophy associated with homocysteine and cognitive decline. PMID 24927906
-
Douaud etal 2013 Preventing Alzheimer's disease-related gray matter atrophy by B-vitamin treatment. PMID 23690582
-
Durga etal, 2007 Effect of 3-year folic acid supplementation on cognitive function in older adults in the FACIT trial:... PMID 17240287
-
de Jager etal, 2012 Cognitive and clinical outcomes of homocysteine-lowering B-vitamin treatment in mild cognitive impairment: A randomized controlled trial. PMID 21780182
-
Smith etal, 2010 Homocysteine-lowering by B vitamins slows the rate of accelerated brain atrophy in mild cognitive impairment: A randomized controlled trial. PMID 20838622
-
Harris etal, 2015 Improved blood biomarkers but no cognitive effects from 16 weeks of multivitamin supplementation in healthy older adults PMID 25996285
-
Zhang etal, 2016 Decreased levels of vitamin B12 in aging, autism and schizophrenia. PMID 26799654
-
Garcua-Minguillan etal, 2014 Riboflavin status modifies the effects of methylenetetrahydrofolate reductase (MTHFR) and methionine synthase reductase (MTRR) polymorphisms on homocysteine PMID 25322900
-
Shankle etal, 2016 CerefolinNAC therapy of hyperhomocysteinemia delays cortical and white matter atrophy in Alzheimer's disease and cerebrovascular disease PMID 27567825
-
Blundo etal, 2011. Vitamin B12 deficiency associated with symptoms of frontotemporal dementia. PMID 20927562
-
Katuoka etal, 1997 A case of vitamin B12 deficiency with broad neurological disorders and canities. PMID 9125735
-
Ikeda etal, 1992 Treatment of Alzheimer-type dementia with intravenous mecobalamin. PMID 1638504
-
Olivier etal, 2009 Melatonin promotes oligodendroglial maturation of injured white matter in neonatal rats. PMID 1638504
-
Villapol etal, 2011 Melatonin promotes myelination by decreasing white matter inflammation after neonatal stroke PMID 1638504
-
Turgut and Kaplan 2011 Effects of melatonin on peripheral nerve regeneration PMID 17101822
-
Miller etal 2014 Antenatal antioxidant treatment with melatonin to decrease newborn neurodevelopmental deficits and brain injury.. PMID 17101822
-
Onger etal 2017 Possible effects of some agents on the injured nerve in obese rats:..... PMID 17101822
-
Higgins and Flicker, 2003 Lecithin for dementia and cognitive impairment. PMID 12917896
-
Cardoso etal, 2018 Supranutritional Sodium Selenate supplementation delivers Selenium to the central nervous system:... PMID: 30215171
-
Moriyama etal, 1996 Effects of dietary phosphatidylcholine on memory in memory deficient mice with low brain acetylcholine. PMID: 8569416
-
Jiang etal, 2016 Partial BACE1 reduction in a Down syndrome mouse model blocks Alzhemier-related endosomal anomalies and cholinergic neurodegeneration: role of APP-CTF. PMID: 26923405
-
Lombardo and Maskos, 2015 Role of nicotinic acetylcholine receptor in Alzheimer's disease pathology and treatment. PMID 25514383
-
Groth etal, 2014 Atrophy of the cholinergic basal forebrain in dementia with Lewy bodies and Alzheimer's disease dementia. PMID 25059393
-
Lin etal, 2013 Chronic rapamycin restores brain vascular integrity and function through NO synthase activation and improves memory in symptomatic mice modeling Alzheimer's disease. PMID 23801246
-
de la Monte etal, 2000 Role of aberrant nitric oxide synthase-3 expression in cerebrovascular degeneration and vascular-mediated injury in Alzheimer's disease. PMID: 10818490
-
Austin etal, 2010 Endothelial nitric oxide modulates expression and processing of amyloid precursor protein. PMID 21127294
-
Boyle etal, 2015 Physical activity, body mass index, and brain atrophy in Alzheimer's Disease. PMID: 25248607
-
Ryuno etal, 2016 Differences in the association between high blood pressure and cognitive functioning..... PMID: 27009579
-
Wlodek and Gonzales, 2003 Decreased energy levels can cause and sustain obesity.. PMID: 14559057
-
Smith etal, 2010 Aerobic exercise and neurocognitive performance: a meta-analytic review of randomized controlled trials .... PMID: 20223924
-
Bossers eatl, 2015 A 9-week aerobic and strength training program improves cognitive and motor function in patients with dementia. PMID: 25648055
-
Maes etal, 2009 Lower plasma Coenzyme Q10 in depression: a marker for treatment resistance and chronic fatigue in depression... PMID: 20010493
-
Palmer and DeKosky, 1993. Monoamine neurones in aging and Alzheimer's disease. PMID: 19197069
-
McNab etal, 2009 Changes in cortical dopamine D1 receptor binding associated with cognitive training.. PMID: 19197069
-
Annweiler 2016 Vitamin D in dementia prevention PMID 27116242
-
Paglia etal 2016 Distinctive pattern of serum elements during the progression of Alzheimer's disease PMID 26957294
-
Smorgon etal 2004 Trace elements and cognitive impairment: an elderly cohort studyMID 15207438
-
Van der Jeugd etal 2018 Reversal of memory and neuropsychiatric symptoms and reduced tau pathology by selenium .... PMID 29691439
-
Taking Vitamin D Could Help Prevent Dementia - Neuroscience News
Copyright © 2018 B12 Oils. All Rights Reserved.
Reproduction in whole or in part in any form or medium without express written
permission is prohibited